Loading...

What is the sympathetic chain?
The sympathetic chain is a bundle of nerve fibres that runs from the base of the skull up to the tail bone. In the chest, it runs in the back, along the ribs.
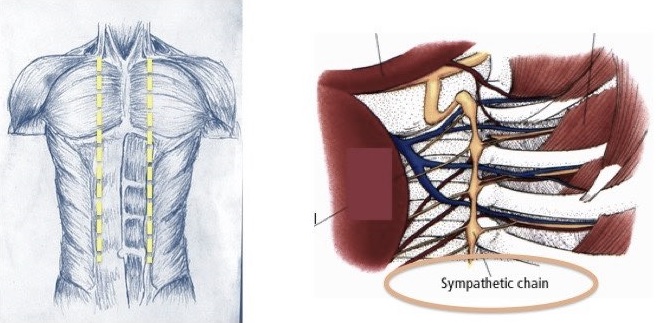
The 2nd sympathetic ganglion (T2) supplies the face (and palms to some extent) and is usually blocked as a treatment for facial hyperhidrosis or blushing. The 3rd and 4th sympathetic ganglia (T3, T4) are mainly responsible for palmar sweating, though the the 2nd sympathetic ganglion (T2) and the Stellate ganglion (C7-T1) innervates in 10% of the population. T5 (and T4 to some extent) is concerned with sweating in the axilla (armpit).

What is open sympathectomy?
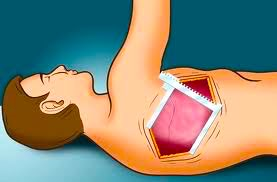
Open surgical methods have been described for sweaty palms since the 1940�s. These involved opening up of the chest wall to get access to the sympathetic chain of nerve fibres. There were difficulties in access and technique. Large incisions meant more pain, discomfort and healing time. Patients took long to recover and resume normal activity.
These procedures were more morbid with potentially hazardous complications.
What is Endothoracic sympathectomy (ETS)?
Endothoracic sympathectomy is minimally invasive surgical procedure that is now considered the gold standard of treatment for sweaty palms. It is an effective treatment modality for primary palmar hyperhidrosis as compared to all other treatment options and is considered the gold standard of treatment for the same. It is routinely performed in as a 'short-stay' procedure with 24 hours hospitalisation.
How is ETS performed?
-
The procedure is performed under general anesthesia. This requires an overnight fasting. The armpits need to be shaved before the procedure.
-
Single lung ventilation allows one lung to be collapsed at a time to give good access to the sympathetic chain. This is the first step of the procedure where the anesthetist deflates the lung on one side.
-
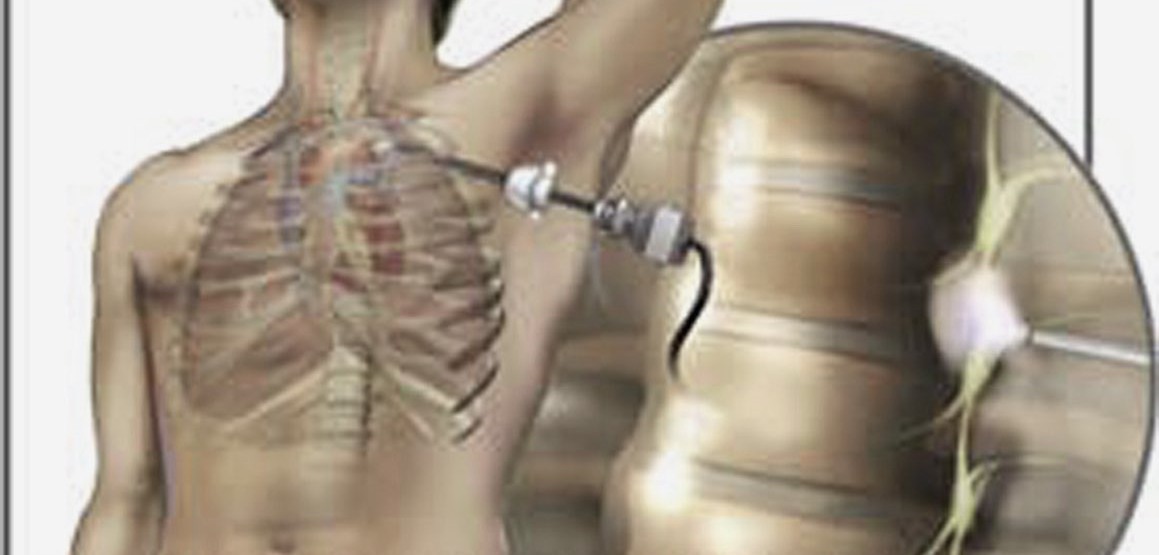
A small skin puncture is made and a 3-5mm cannula is introduced in the chest. A video telescope is put into this cannula to visualise the interior of the chest.
-
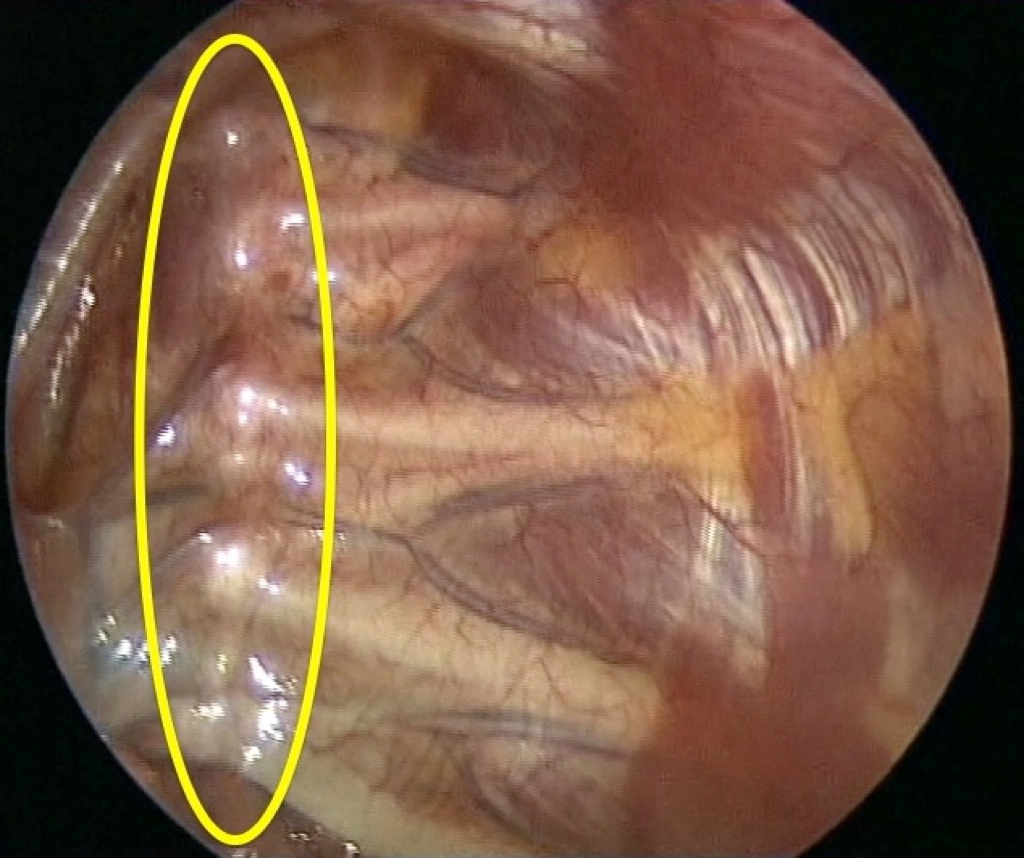
A second cannula is also inserted to allow another instrument into the chest. The sympathetic chain is identified. and ablated (cut or clipped) at the desired levels.
-
The sympathetic chain is then blocked or ablated (cut or clipped) at the desired levels. The sympathetic chain is commonly blocked at the level of the third (R3) and fourth (R4) ribs for palmar hyperhidrosis. The second rib (R2) is blocked in case of facial hyperhidrosis and the fifth rib (R5) for axillary hyperhidrosis. The procedure is always performed on the opposite side as well, as there is cross connection of nerve innervations across the midline. Some centres offer them one at a time, but we always recommend both in the same sitting. This has the benefits of a single hospitalisation and anesthesia with immediate relief of symptoms without adding too much in terms of morbidity.






What is the recovery from ETS?
Surgery offers immediate relief with the patient waking up from anesthesia with dry hands. The effect is usually permanent. There is a good overlap of functions of the sympathetic chain, so there are no know long-term side effects of the sympathectomy. Most patients are discharged the following day. The procedure is usually well accepted with good patient satisfaction and improved quality of life.
What are the benefits of ETS?
ETS offers the following benefits:
-
Small Scars
-
Better cosmesis
-
Reduced post-op pain
-
Shorter hospitalization
-
Earlier recovery and return to normal activity and work
-
Reduced morbidity and mortality
-
Immediate and usually permanent results
-
Often, patients will also show an improvement in sweating from the feet and armpits.

What are the postoperative complications of ETS?
No operation is without risk and can include anesthetic complications, bleeding, infection and damage to surrounding organs. Complications specific to ETS are rare, but include:

Compensatory sweating: Once the palms (and soles) are dry, the body will need to sweat from other areas to lose the excess heat and maintain the normal body temperature. Most patients experience compensatory sweating from other parts of the body like the trunk, face, lower limbs etc. This is usually mild and less disturbing than the primary problem. This can sometimes manifest as severe sweating from some part of the body (e.g. back, hips etc) that may make the patient regret the procedure. It is difficult to predict this outcome preoperatively and all patients must be aware of this before embarking on ETS. Restricting the number of levels cut and sparing the first 2 levels has found to be more acceptable.
Residual Symptoms: ETS will give excellent results in over 90% cases. In the remaining, symptoms may partially or fully persist for unexplained reasons. These include anatomical variations, aberrant nerve pathways etc.
Recurrence: occurs in 1-2% patients. This may be mild, usually in situations like heavy physical activity, hot weather or other stressful situations. A redo surgery is seldom required if symptoms are severe.
Heart rate changes: Reduction in heart rate may occur in a few cases, but has no physiologic significance and no long term effect on the cardiovascular function.
Pneumothorax: Sometimes air remains inside the chest after surgery. This is usually insignificant and gradually gets absorbed. Rarely, a small drainage tube may be required to be placed in the chest to let the air out.
Gustatory sweating: Patients experience increased sweating while eating or smelling certain foods. This is extremely rare.
Horner’s syndrome: This is also known as ‘droopy eye syndrome’ and occurs due to damage to the C7 ganglion if the sympathetic chain is attempted to be cut high at the level of the Stellate ganglion (C7-T1). It is very rare, as it is common practice to spare T1.